1186
Introduction of Targeted Rapid Knee MRI exam using T2 Shuffling into Clinical Practice: Retrospective Analysis on Image Quality, Charges, and Scan Time1Electrical Engineering and Computer Sciences, University of California, Berkeley, Berkeley, CA, United States, 2MR Applications & Workflow, GE Healthcare, Menlo Park, CA, United States, 3Radiology, Stanford University, Stanford, CA, United States, 4Radiology, Lucile Packard Children’s Hospital, Palo Alto, CA, United States, 5Intel Labs, Santa Clara, CA, United States, 6Intel Labs, Hillsboro, OR, United States
Synopsis
Volumetric fast spin echo (FSE) of the knee using T2 Shuffling (T2Sh) has previously been described as comparable to traditional 2D imaging. T2Sh has the added advantage of being a rapid single-scan 4D multi-plane reformattable sequence for pediatric knee examinations. This study investigates the feasibility and effectiveness of a targeted rapid pediatric knee MRI exam after introduction into clinical practice, with the goal of reducing cost and enabling same-day MRI access.
Introduction
Magnetic resonance imaging (MRI) is commonly used to evaluate musculoskeletal pathologies. Despite its advantages, MRI of the pediatric knee presents several challenges due to requirements for sub-millimeter spatial resolution and multiple contrasts$$$^{1,2}$$$, leading to lengthy scan and exam times. The long exams often lead to a high cost, limiting the value of the MRI exam in the context of clinical care. Volumetric fast-spin-echo (3D FSE) alternatives to the standard knee protocol are attractive because they theoretically provide isotropic resolution and larger slice coverage, enabling multi-planar reformats and eliminating the need to separately scan at multiple orientations with additional technologist planning$$$^{3-8}$$$. The primary challenge with 3D FSE acquisitions is the tradeoff between scan time and image blurring due to long echo trains$$$^{3,9}$$$.
Recently, an acquisition based on 3D FSE was proposed that permits volumetric reconstruction of images with contrast varying from proton-density (PD) weighting to increasing T2 weighting$$$^7$$$. This seven-minute scan, termed T2 Shuffling (T2Sh), uses ideas from compressed sensing$$$^10$$$ to accelerate the acquisition and mitigate blurring due to T2 decay by accounting for relaxation behavior. A prior study with 30 consecutive patients investigating a single sequence protocol using T2Sh, compared against the conventional protocol, indicated that missing clinically relevant pathology is unlikely$$$^8$$$. The use of T2Sh in a targeted exam is attractive because it provides images at multiple clinical contrasts, obviating the need for numerous conventional 2D scans$$$^11$$$. The purpose of this study is to investigate the feasibility and effectiveness of a targeted rapid pediatric knee MRI exam after introduction into clinical practice, with the goal of reducing cost and enabling same-day MRI access.
Materials and Methods
Results
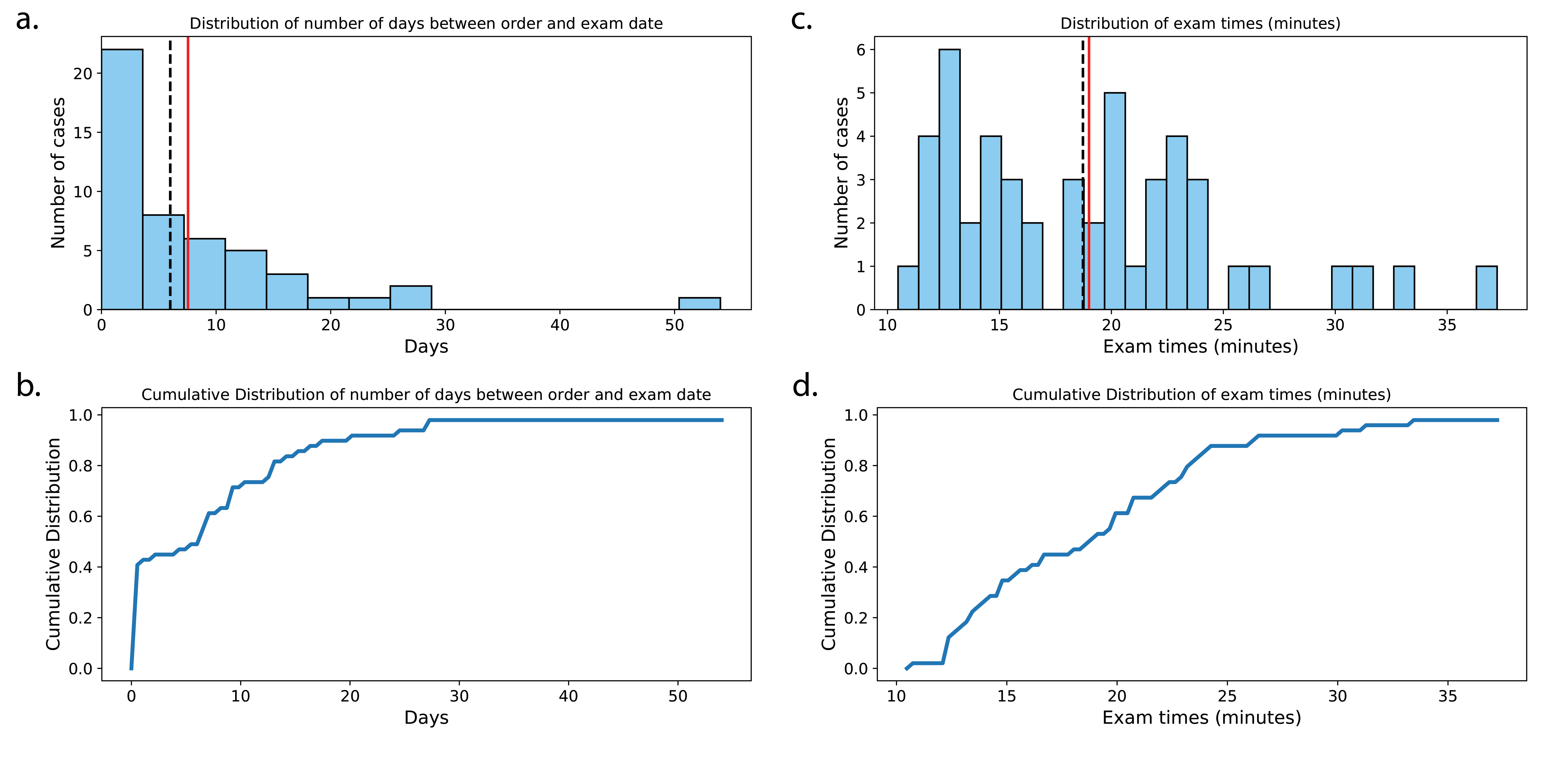
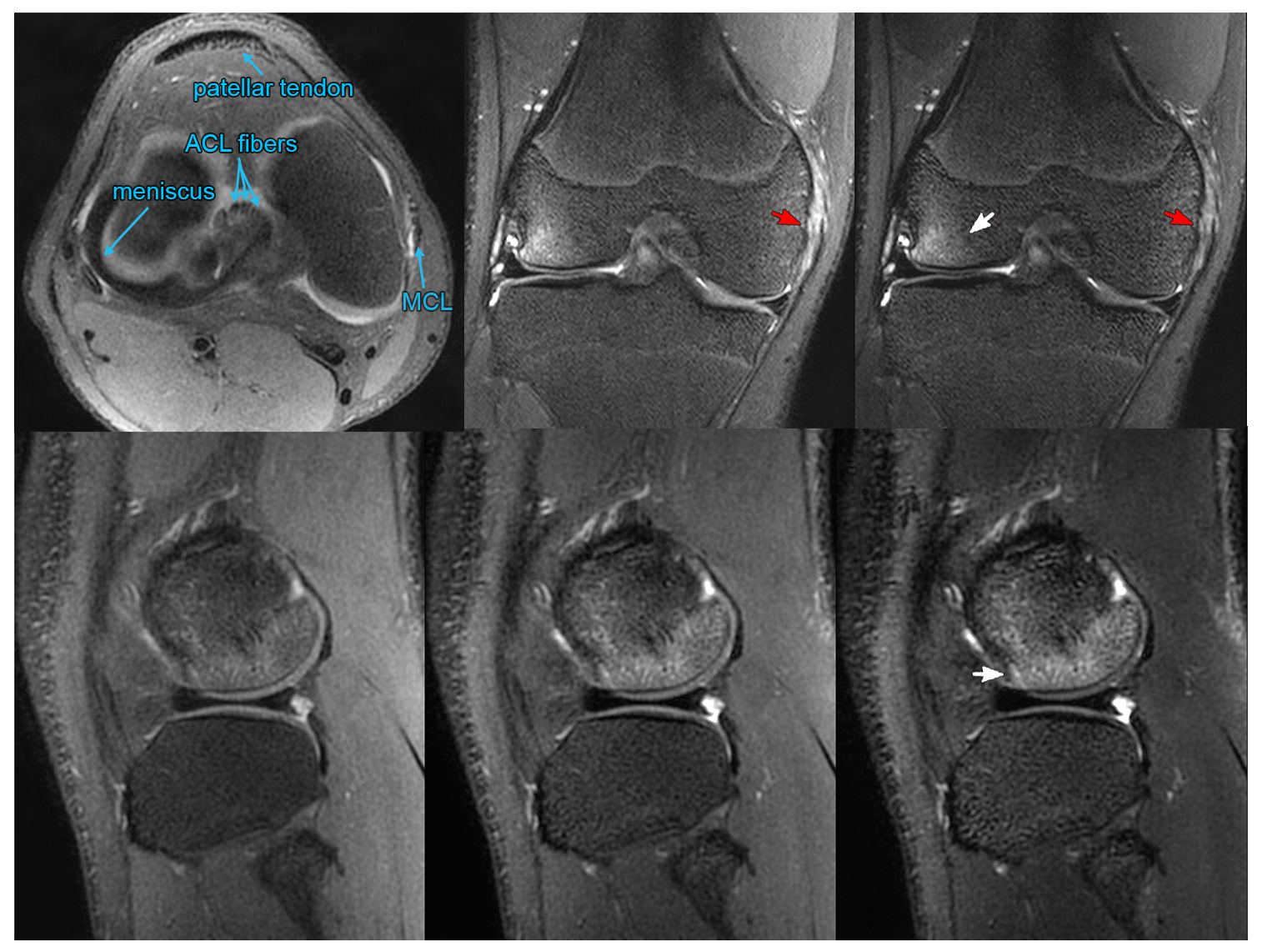
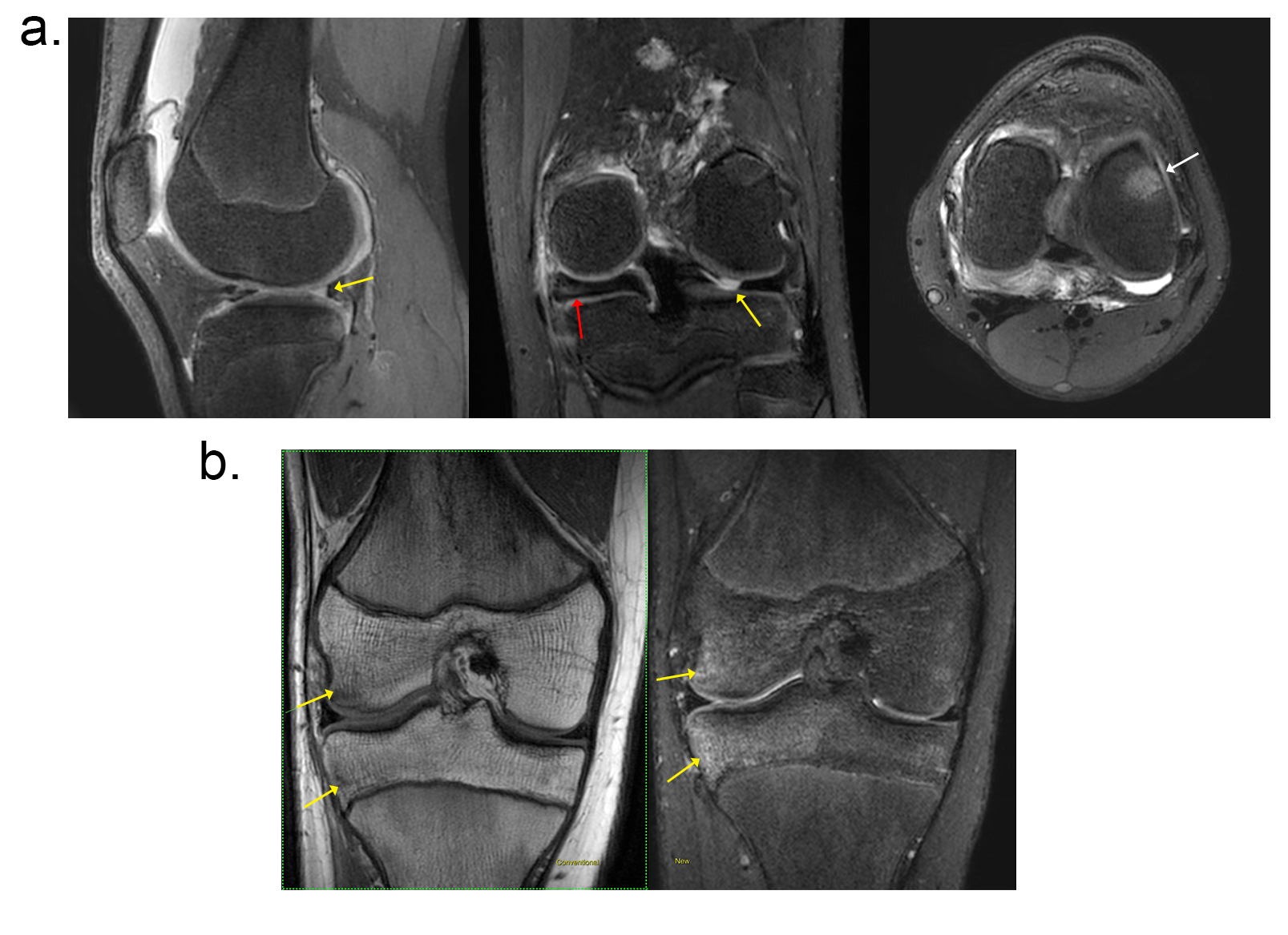
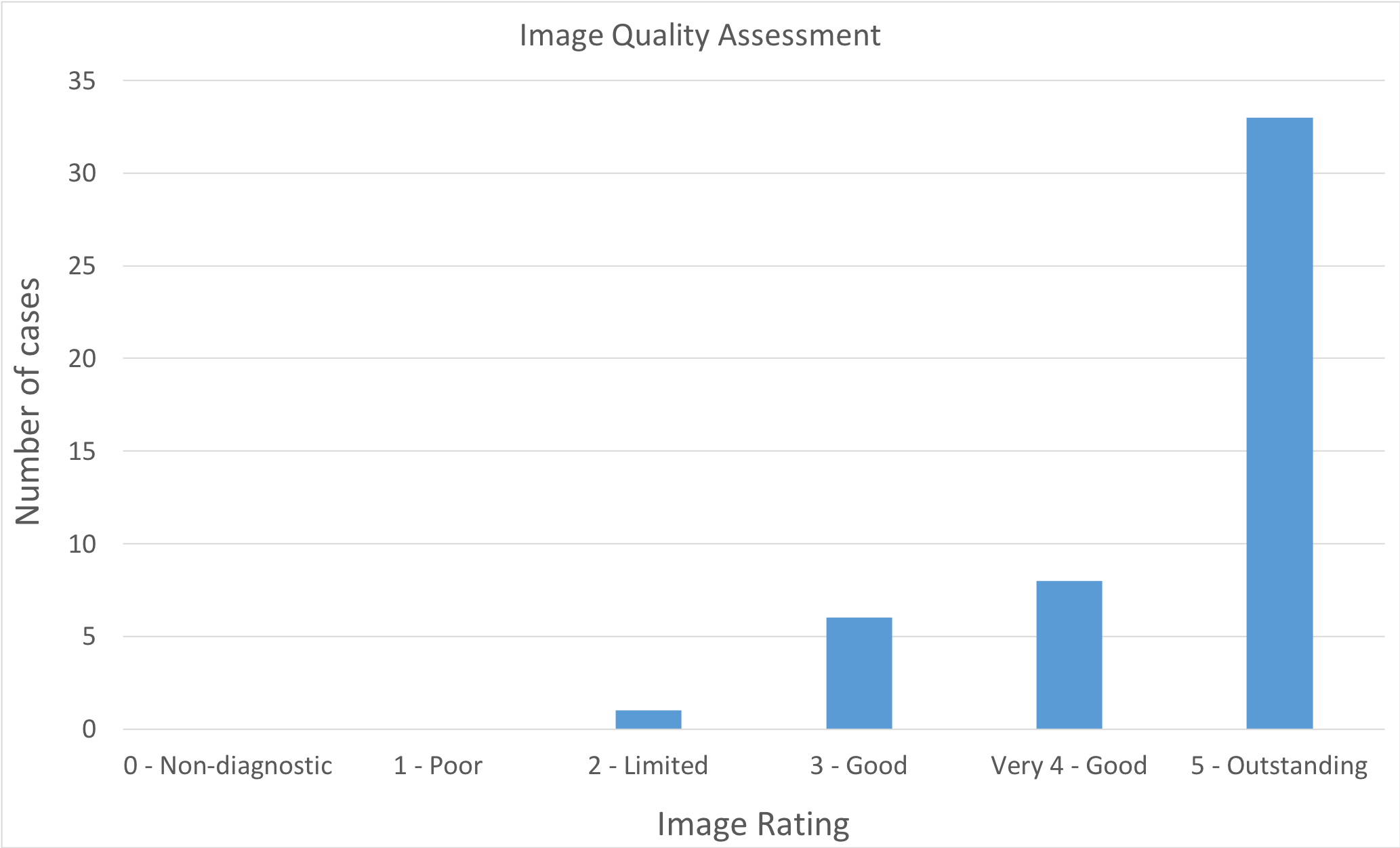
Of the 47 subjects, 18 completed the exam on the same day as their referral (Figure 2). Median time from registration to exam completion was 18.7 minutes. Median end-to-end reconstruction time for the T2 Shuffling sequence was reduced from 18.9 minutes to 95 seconds using the distributed implementation. Technical fees charged for the targeted exam were one third that of the routine clinical knee exam. Figure 3 shows a 14-year-old male evaluated for internal derangement of the knee. The T2Sh image formatted into axial PD weighting is annotated to demarcate the patellar tendon, ACL fibers, meniscus, and MCL. Edema and partial tearing/sprain of the MCL is visualized in the T2Sh coronal and sagittal images. Figure 4 shows two patients referred for meniscal tear. Image quality assessment is shown in Figure 5. Greater than 85% of the cases were rated as very good to outstanding. No exams were deemed non-diagnostic or poor quality. No subject had to return for additional imaging.Discussion
As the imaging time for the targeted exam was reduced compared to the conventional knee MRI, a reduced charge modifier code was used for insurance billing, lowering the technical fees to one third of the conventional knee MRI fee. In this study, about 38% of the exams were completed on the same day. In comparison, our institution had no instances of same-day scheduling for routine knee MRI prior to the introduction of the targeted knee exam. The distributed reconstruction enabled a streamlined workflow for the technologists, as the images were available on the scanner console before the T1 scan finished.
A limitation of this study was that arthroscopic data was not available to corroborate the MRI findings, though the focus of this study was on scheduling feasibility. A second limitation was the relatively small number of participants. The targeted knee exam was intentionally limited to a small subset of clinical indications and insurance pre-authorizations during its initial implementation, but further evaluation is required at a multi-site level.
Conclusion
The targeted knee MRI exam is feasible and reduces imaging time, cost, and barrier to same-day MRI access for pediatric patients.Acknowledgements
We thank the following funding sources: National Institutes of Health (NIH) grants R01EB009690, P41RR09784; Sloan Research Fellowship; Bakar Fellowship; GE Healthcare, and Intel Labs.References
- Laor T, Jaramillo D. Pediatric musculoskeletal MRI: basic principles to optimize success. Pediatr Radiol 2008;38(4): 379-391.
- Strouse P, Koujok K. Magnetic resonance imaging of the pediatric knee. Top Magn Reson Imaging 2002; 3(4):277-294.
- Mugler JP. Optimized three-dimensional fast-spin-echo MRI. J Magn Reson Imaging 2014;39(4):745-767.
- Fritz J, Raithel E, Thawait GK, Gilson W, Papp DF. Six-Fold Acceleration of High-Spatial Resolution 3D SPACE MRI of the Knee Through Incoherent k-Space Undersampling and Iterative Reconstruction-First Experience. Invest Radiol 2016;51(6):400-409.
- Kijowski R, Rosas H, Samsonov A, King K, Peters R, Liu F. Knee imaging: Rapid three-dimensional fast spin-echo using compressed sensing. J Magn Reson Imaging 2017;45(6):1712-1722.
- Fritz J, Ahlawat S, Fritz B, et al. 10‐Min 3D Turbo Spin Echo MRI of the Knee in Children: Arthroscopy‐Validated Accuracy for the Diagnosis of Internal Derangement. J Magn Reson Imaging 2018; in press. doi: 10.1002/jmri.26241.
- Tamir JI, Uecker M, Chen W, et al. T2 shuffling: Sharp, multicontrast, volumetric fast spin-echo imaging. Magn Reson Med 2016;77(1):180-195.
- Bao S, Tamir JI, Young JL, et al. Fast comprehensive single-sequence four-dimensional pediatric knee MRI with T2 shuffling. J Magn Reson Imaging 2016;45(6):1700-1711.
- Busse RF, Brau ACS, Vu A, et al. Effects of refocusing flip angle modulation and view ordering in 3D fast spin echo. Magn Reson Med 2008;60(3):640-649
- Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med 2007;58(6):1182-1195.
- Tamir JI, Anderson MJ, Turek J, Roh A, Alley MT, Lustig M, Vasanawala SS. Targeted Rapid MRI Exams and Reconstructions using T2 Shuffling. ISMRM-RSNA Co-Provided Workshop on High-Value MRI, Washington, DC, 2008.
- Anderson MJ, Tamir JI, Turek J, et al. Clinically Deployed Distributed Magnetic Resonance Imaging Reconstruction: Application to Pediatric Knee Imaging. Arxiv 2018; preprint. doi: arXiv:1809.04195v1.
Figures